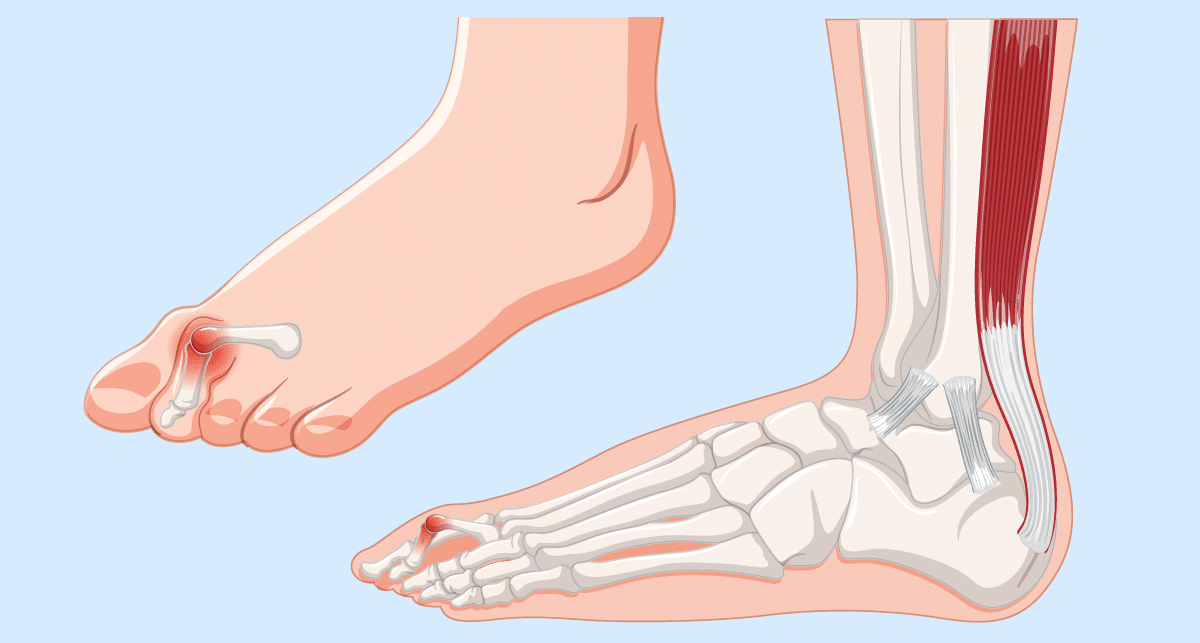
Hammer toe is a deformity affecting one of the smaller toes, most commonly the second, third or fourth toe. The middle joint of the toe bends abnormally, causing the toe to curl downward so that it resembles the shape of a hammer.
In the early stages the toe may still be flexible and can be straightened with gentle pressure. Over time, however, the soft tissues around the joint tighten and the deformity can become fixed. When this happens the toe may rub against footwear, leading to pain, calluses or corns.
Hammer toe is a common foot condition and can affect people of all ages, although it is seen more frequently in adults and in those who spend long periods standing, walking or wearing restrictive footwear.
Who Gets Hammer Toe?
Hammer toe can develop gradually over time and is often the result of an imbalance between the muscles, tendons and ligaments that normally keep the toes straight.
It is more commonly seen in:
Adults over the age of 40
People who regularly wear tight or narrow shoes
Women, particularly those who frequently wear high heels
Individuals with certain foot shapes or structural issues
Athletes and people who are on their feet for long periods can also develop hammer toe, particularly if footwear does not allow enough space for the toes.
Predisposing Factors
Several factors can increase the likelihood of developing hammer toe. These include structural foot problems, footwear choices and certain medical conditions.
Common predisposing factors include:
Tight or ill-fitting footwear – Shoes with a narrow toe box can force the toes into a bent position over time.
High-heeled shoes – These shift weight onto the front of the foot and increase pressure on the toes.
Foot structure – Long second toes, flat feet, or high arches may contribute.
Bunions (hallux valgus) – A bunion can push the second toe out of alignment.
Previous foot injuries – Trauma to the toe or forefoot can alter joint alignment.
Neuromuscular conditions – Conditions such as rheumatoid arthritis, diabetes-related nerve problems, or neurological disorders can affect muscle balance in the foot.
Often there is not a single cause but rather a combination of these factors.
Symptoms of Hammer Toe
Symptoms usually develop gradually and may worsen over time if the toe becomes more rigid.
Common symptoms include:
A toe that bends downward at the middle joint
Pain or discomfort in the affected toe
Corns or calluses on the top of the toe from shoe pressure
Pain in the ball of the foot
Difficulty finding comfortable footwear
Redness, swelling or irritation around the joint
In the early stages symptoms may only occur when wearing certain shoes or after long periods of walking or standing.
Aggravating Factors
Certain activities and footwear choices can make hammer toe symptoms worse.
Common aggravating factors include:
Tight or narrow shoes
High heels
Long periods of walking or standing
Sporting activities that place pressure on the forefoot
Shoes with stiff uppers that rub on the bent toe
Over time, repeated friction and pressure can lead to painful corns or skin irritation.
Assessment
If hammer toe is causing persistent discomfort or affecting daily activities, an assessment by a specialist is recommended.
During your consultation at London Bridge Orthopaedics, your clinician will:
Discuss your symptoms and how they developed
Ask about footwear, activity levels and previous foot problems
Examine the shape and movement of the toes
Assess whether the toe deformity is flexible or fixed
Look for associated problems such as bunions, calluses or joint stiffness
Understanding whether the deformity is flexible or rigid helps guide treatment decisions.
Diagnosis
Hammer toe is usually diagnosed through a clinical examination.
In some cases, imaging such as X-rays may be recommended.
These can help:
Assess the alignment of the toe joints
Identify arthritis within the joint
Evaluate other forefoot problems that may be contributing to the deformity
Imaging is particularly helpful when surgical treatment is being considered.
Conditions With Similar Symptoms (Differential Diagnosis)
Several other forefoot conditions can cause similar symptoms or toe deformities.
These may include:
Claw toe deformity
Mallet toe (where only the tip joint bends)
Bunion-related toe deformity
Metatarsalgia (pain in the ball of the foot)
Arthritis of the toe joints
A specialist assessment helps ensure the correct diagnosis and the most appropriate treatment plan.
Non-Surgical (Conservative) Treatment
In many cases, especially when the deformity is still flexible, symptoms can be managed without surgery.
Conservative treatments aim to reduce pressure on the toe, relieve discomfort and slow progression of the deformity.
These may include:
Footwear modification
Wearing shoes with a wider toe box can reduce pressure on the toes and prevent rubbing. Avoiding tight shoes and high heels is often helpful.
Padding and orthotics
Protective pads or silicone sleeves can reduce friction over the toe. Custom orthotics may help redistribute pressure across the forefoot and improve foot mechanics.
Exercises and stretching
Gentle toe exercises may help maintain flexibility in the early stages.
Management of corns and calluses
Regular care from a podiatrist can reduce painful areas of thickened skin caused by shoe pressure.
While these measures can relieve symptoms, they do not usually correct an established toe deformity.
When Is Surgery Considered?
Surgery may be recommended when:
Pain persists despite conservative treatment
The toe deformity becomes rigid
Corns or calluses repeatedly develop
Footwear becomes difficult or painful to wear
The deformity interferes with walking or daily activities
Modern surgical techniques are generally very effective at correcting hammer toe and relieving symptoms.
The aim of surgery is to straighten the toe, restore a more normal alignment and remove the source of pressure within footwear.
Surgical Treatment Options
The most appropriate surgical technique depends on the severity of the deformity, whether the toe is flexible or rigid, and whether other forefoot problems are present.
Tendon Release or Tendon Transfer
In early or flexible hammer toe deformities, surgery may involve releasing or repositioning the tendons that are pulling the toe into a bent position.
This procedure allows the toe to return to a straighter alignment while preserving joint movement.
It is usually performed as a day-case procedure and recovery is relatively quick – 4-8 weeks.
Joint Realignment (Arthroplasty)
For more established deformities, part of the small joint in the toe may be reshaped to allow the toe to straighten.
This procedure removes a small section of bone from the joint, relieving stiffness and allowing the toe to sit in a more natural position.
The toe may be temporarily supported with a small pin during healing, which is typically removed after a few weeks.
Joint Fusion (Arthrodesis)
In more severe or rigid hammer toe deformities, fusing the joint may provide the most reliable correction.
During this procedure the small joint in the toe is permanently straightened and fused in position. Although the joint no longer moves, the toe sits straight and pain from the deformity is usually resolved.
Fusion procedures are commonly used when the joint has become stiff or arthritic.
Combined Procedures
Hammer toe often occurs alongside other forefoot problems such as bunions or instability in the ball of the foot.
In these situations, surgeons may correct multiple issues at the same time. Addressing the underlying cause of the deformity can improve long-term results and reduce the risk of recurrence.
Recovery After Surgery
Hammer toe surgery is usually performed as a day-case procedure, meaning patients go home the same day.
Recovery typically involves:
Wearing a protective post-operative shoe for several weeks
Keeping the foot elevated in the early stages to reduce swelling
Gradual return to normal footwear
Light activities after a few weeks, with a full return to normal activity over a few months
Your surgeon will provide detailed guidance on post-operative care and rehabilitation.
Outcomes
Surgery for hammer toe is generally very successful in relieving pain and improving toe alignment.
Most patients experience:
Significant reduction in pain
Improved comfort in footwear
A straighter, more natural toe position
Improved walking comfort
As with any surgery there are potential risks, but these are relatively uncommon and will be discussed during your consultation.
When appropriately selected, surgical correction of hammer toe can provide lasting relief and allow patients to return to normal daily activities with greater comfort.
Frequently Asked Questions
Can hammer toe correct itself without treatment?
In the early stages, when the toe is still flexible, symptoms can sometimes improve with simple measures such as wearing wider shoes, using protective padding and performing gentle toe exercises. However, once the deformity becomes fixed, it is unlikely to correct itself without medical treatment.
Is hammer toe painful?
Hammer toe can be painful, particularly when the bent joint rubs against footwear. This can lead to pressure points, corns or calluses on the top of the toe. Some people also experience discomfort in the ball of the foot due to changes in weight distribution while walking.
When should I see a specialist about hammer toe?
You should consider seeing a specialist if the toe deformity is becoming more noticeable, if pain is affecting your daily activities, or if it is becoming difficult to find comfortable shoes. Early assessment can help prevent the condition from worsening and may allow more conservative treatment options.
Is hammer toe surgery painful?
Hammer toe surgery is usually performed as a day-case procedure and is typically well tolerated. Some discomfort and swelling are expected during the early recovery period, but this is usually manageable with simple pain relief and rest. Most patients notice significant improvement in symptoms once the toe has healed.
How successful is hammer toe surgery?
Surgery for hammer toe is generally very successful at correcting the deformity and relieving pain. Most patients experience improved comfort in footwear and better toe alignment. When the underlying cause of the deformity is also addressed, the long-term results are usually very good.
London’s Leading Specialist Orthopaedic Consultants
We are a group of established consultants who care about our patients. We cover all the subspecialty areas of orthopaedics:
The tennis serve is one of the most explosive movements in all of sport — the shoulder rotates internally at speeds approaching 2,500 degrees per second, generating power from a joint barely the size of a golf ball. Mr Simon Owen-Johnstone, Consultant Shoulder & Elbow Surgeon, explains why your shoulder is built for mobility over stability, why serve-related pain is rarely the shoulder’s fault, and how small changes could transform both your game and your long-term shoulder health.
Wrist pain from padel, tennis and gym training is becoming increasingly common. As more people take up racket sports, strength training and high-intensity fitness, hand and wrist specialists are seeing a growing number of patients with overuse injuries, tendon problems and acute trauma.