Rotator cuff tears are a common cause of shoulder pain and dysfunction, particularly in individuals over 40 or those involved in repetitive overhead activities. The rotator cuff is a group of muscles and tendons that stabilise the shoulder joint and facilitate arm movement. A tear in one or more of these tendons can significantly limit mobility and strength, affecting daily activities and quality of life. Early diagnosis and appropriate management—whether conservative or surgical—can lead to excellent outcomes.
Anatomy of the Shoulder
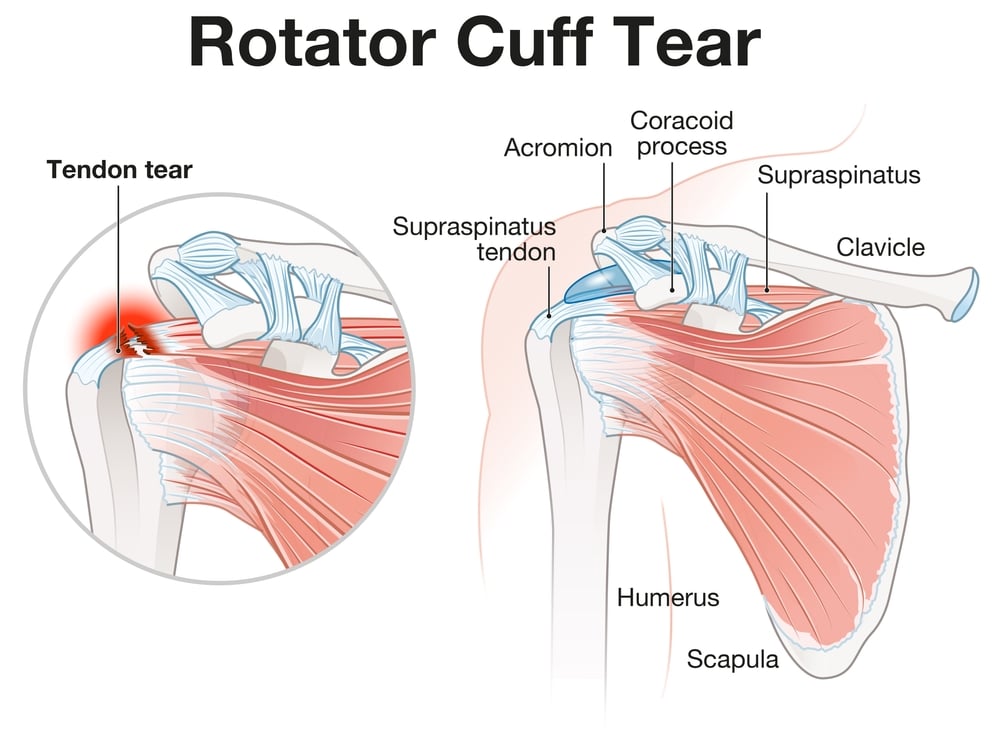
The shoulder is a complex ball-and-socket joint comprising the humerus (upper arm bone), scapula (shoulder blade), and clavicle (collarbone). The rotator cuff is made up of four muscles: supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles converge into tendons that attach to the humeral head, stabilising the shoulder and enabling movements such as lifting, reaching, and rotating the arm.
The supraspinatus tendon is the most commonly affected in rotator cuff tears.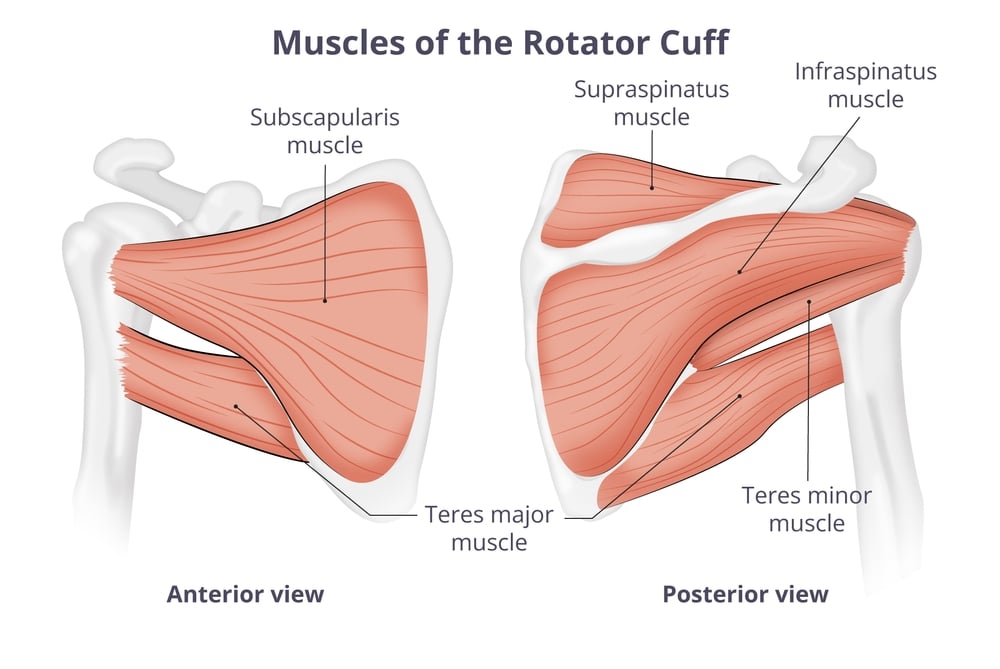
Causes of Rotator Cuff Tears
Rotator cuff tears can develop through two main mechanisms: acute trauma or chronic degeneration, each with distinct contributing factors and typical presentations.
Acute Tears
Acute rotator cuff tears typically occur as a result of a sudden, forceful movement or trauma. Common injury mechanisms include:
- Falling onto an outstretched arm
- Lifting something heavy with a jerking motion
- Sudden pulling or wrenching of the shoulder
- Direct impact to the shoulder in contact sports
These injuries are frequently seen in younger individuals or athletes involved in:
- Contact sports such as rugby, football, or judo
- Overhead sports like tennis, cricket (especially bowling), swimming, volleyball, and baseball
- Weightlifting, particularly exercises involving heavy shoulder loading (e.g., overhead press, clean and jerk)
Degenerative (Chronic) Tears
Degenerative tears are far more common and typically develop gradually over time due to repetitive stress and age-related wear and tear. The risk increases significantly after the age of 40, especially in those with physically demanding jobs or hobbies.
Contributing factors include:
- Repetitive overhead activities (e.g., painting, carpentry, ceiling work)
- Poor posture and shoulder biomechanics
- Chronic shoulder impingement or bony spurs that rub against the tendons
- Reduced blood supply to the tendons with age, impairing natural healing
- Previous shoulder injuries or instability
- Degenerative tears often begin as partial-thickness tears and may slowly progress to full-thickness tears if left untreated. Other risk factors include smoking, high cholesterol, diabetes, and a family history of tendon disease.
Symptoms Rotator Cuff Tears
The symptoms of a rotator cuff tear can vary depending on whether the tear is acute or degenerative, and whether it is partial or full-thickness. The onset may be sudden or gradual, and the severity of symptoms does not always correlate with the size of the tear.
Onset and Progression
- In acute tears, symptoms often begin suddenly, following a distinct injury such as a fall or sudden lift. Patients may feel a sharp pain, sometimes accompanied by a tearing sensation.
- In degenerative tears, symptoms typically develop gradually over weeks or months. Many patients may initially attribute the discomfort to overuse or strain.
Common Symptoms
- Shoulder pain: Often located over the top and side of the shoulder, sometimes radiating down the arm. Pain is typically worse at night, particularly when lying on the affected side, and can disturb sleep.
- Weakness: Patients often report difficulty lifting or rotating the arm, particularly during tasks such as reaching overhead, putting on a jacket, or brushing hair. Overhead strength is typically most affected.
- Limited range of motion: Stiffness or catching may be noticed when lifting the arm, and some may find they cannot move the shoulder fully without assistance.
- Clicking or popping sounds: These may be experienced with certain arm movements and can indicate tendon dysfunction or joint instability.
- Loss of function: More significant tears can lead to noticeable difficulty with everyday tasks such as dressing, reaching high shelves, or driving.
In some chronic cases, patients may not experience significant pain but present primarily with weakness or reduced function.

Diagnosis begins with a detailed medical history and physical examination. Your orthopaedic specialist will assess range of motion, strength, and signs of impingement or instability.
Imaging is usually required to confirm the diagnosis:
- Ultrasound – This is an effective diagnostic tool for assessing tendon tears and dynamic movement
- MRI scan – MRI scans provides detailed images of soft tissues, confirming tear size, location, and muscle quality (atrophy/fatty infiltration)
- X-rays – These are used to rule out arthritis or bone spurs but do not show soft tissues
Differential Diagnosis
Several conditions can mimic a rotator cuff tear, and accurate diagnosis is key to effective treatment.
Other conditions that need to be ruled out include:
Your consultant may perform targeted tests and imaging to rule out these alternative or coexisting diagnoses.
Treatment Options
Treatment depends on the size of the tear, patient age, activity level, symptoms, and functional limitations. Most small or partial-thickness tears can be managed conservatively.
Non-Surgical Treatment
- Physiotherapy: Tailored rehabilitation programmes improve shoulder mechanics, strength, and range of motion.
- Activity modification: Avoiding overhead or aggravating movements may help symptoms settle.
- Pain relief: NSAIDs, ice therapy, and manual therapy.
- Corticosteroid injections: May be used selectively to reduce inflammation and pain, particularly in those with chronic shoulder impingement. This treatment is not used for acute tears.
Many patients experience significant improvement with a structured rehabilitation plan over 8–12 weeks.
Surgical Treatment for Rotator Cuff Tears
Surgery is typically considered for:
- Full-thickness tears in active individuals or those under 65
- Tears that have failed conservative management after 3–6 months
- Acute traumatic tears, especially in younger patients
- Tears associated with significant weakness or loss of function
- Progression in tear size or worsening symptoms on imaging
Arthroscopic rotator cuff repair is the most common surgical approach. It is a minimally invasive procedure where small instruments and a camera are inserted through tiny incisions. The torn tendon is reattached to the bone using suture anchors.
In some cases, open repair or mini-open repair may be necessary, particularly for large or complex tears.
Subacromial decompression or acromioplasty may also be performed during surgery to remove bony spurs or reduce impingement. If the tear is deemed irreparable, other procedures such as superior capsular reconstruction or reverse shoulder replacement may be considered.
Who Benefits from Surgery?
Patients who are physically active, wish to return to sports or manual work, or have ongoing pain and weakness despite conservative therapy are the best candidates for surgery. Timely surgical intervention also helps prevent tendon retraction and muscle atrophy, which can complicate future repair.
Outcomes of Rotator Cuff Surgery
Rotator cuff surgery has a high success rate, especially when performed early in the course of a full-thickness tear. Most patients regain significant shoulder function and return to daily activities. Rehabilitation is crucial and typically involves 4–6 months of physiotherapy, with full recovery often taking 6–12 months. Outcomes may vary based on tear size, tendon quality, and adherence to post-operative rehab.
FAQs
Can a rotator cuff tear heal without surgery?
Partial-thickness tears and some small full-thickness tears can improve significantly with physiotherapy and lifestyle changes. Surgery is not always necessary and is typically reserved for larger or persistent tears.
How long is recovery after rotator cuff surgery?
Full recovery can take 6 to 12 months. Most patients wear a sling for 4–6 weeks post-surgery and begin gradual physiotherapy shortly after to regain motion and strength.
Will I regain full strength in my shoulder after a tear?
Many patients regain good strength and function, though full strength may not return in all cases—especially in chronic or massive tears. Early treatment and rehab improve outcomes.
Is it possible to prevent rotator cuff tears?
While not all tears are preventable, maintaining good shoulder strength, flexibility, and posture, along with avoiding repetitive overhead strain, can reduce your risk.
What happens if a rotator cuff tear is left untreated?
Untreated tears can enlarge over time, leading to increased pain, weakness, and the development of shoulder arthritis (cuff tear arthropathy). Early assessment is advised if symptoms persist.





