The tennis serve is one of the fastest and most demanding movements in sport.
Your shoulder is designed for mobility rather than stability, making it vulnerable to injury.
Shoulder pain rarely has one single cause – it’s usually a combination of technique, strength, flexibility, workload and recovery.
Most shoulder problems improve without surgery when diagnosed early and treated with the right rehabilitation.
A collaborative approach involving surgeons, sports physicians and physiotherapists often delivers the best outcomes.
Small changes to your serve mechanics and training programme can make a huge difference to performance and injury prevention.
The Fastest movement you perform… without being in a car
If someone asked you what the most explosive movement in sport is, you might think of a rugby tackle, a cricket fast bowler or a golf drive.
Yet the humble tennis serve deserves a place right at the top of that list.
Professional players routinely accelerate the racket head to over 120 mph, with elite serves exceeding 150 mph.
The shoulder rotates internally at speeds approaching 2,500 degrees per second – one of the fastest movements ever recorded in the human body!
That’s extraordinary.
It’s also slightly terrifying when you stop to think that all of this force is generated by a joint about the size of a golf ball balancing on what is effectively a very shallow tee.
It’s a remarkable feat of engineering. But, like any finely tuned machine, things can start to creak if one part isn’t working quite as it should.
Your shoulder wasn’t built for tennis… but it’s remarkably good at it
One of my favourite analogies is to think of the shoulder as a Formula One racing car.
It’s incredibly fast.
It’s beautifully engineered.
But it requires constant maintenance.
Unlike your hip, which sits securely inside a deep socket, the shoulder sacrifices stability in favour of movement.
That freedom allows us to serve, throw, swim and reach overhead, but it also means the surrounding muscles, tendons and ligaments have to work incredibly hard to keep everything centred.
During a tennis serve, almost every structure around the shoulder is involved.
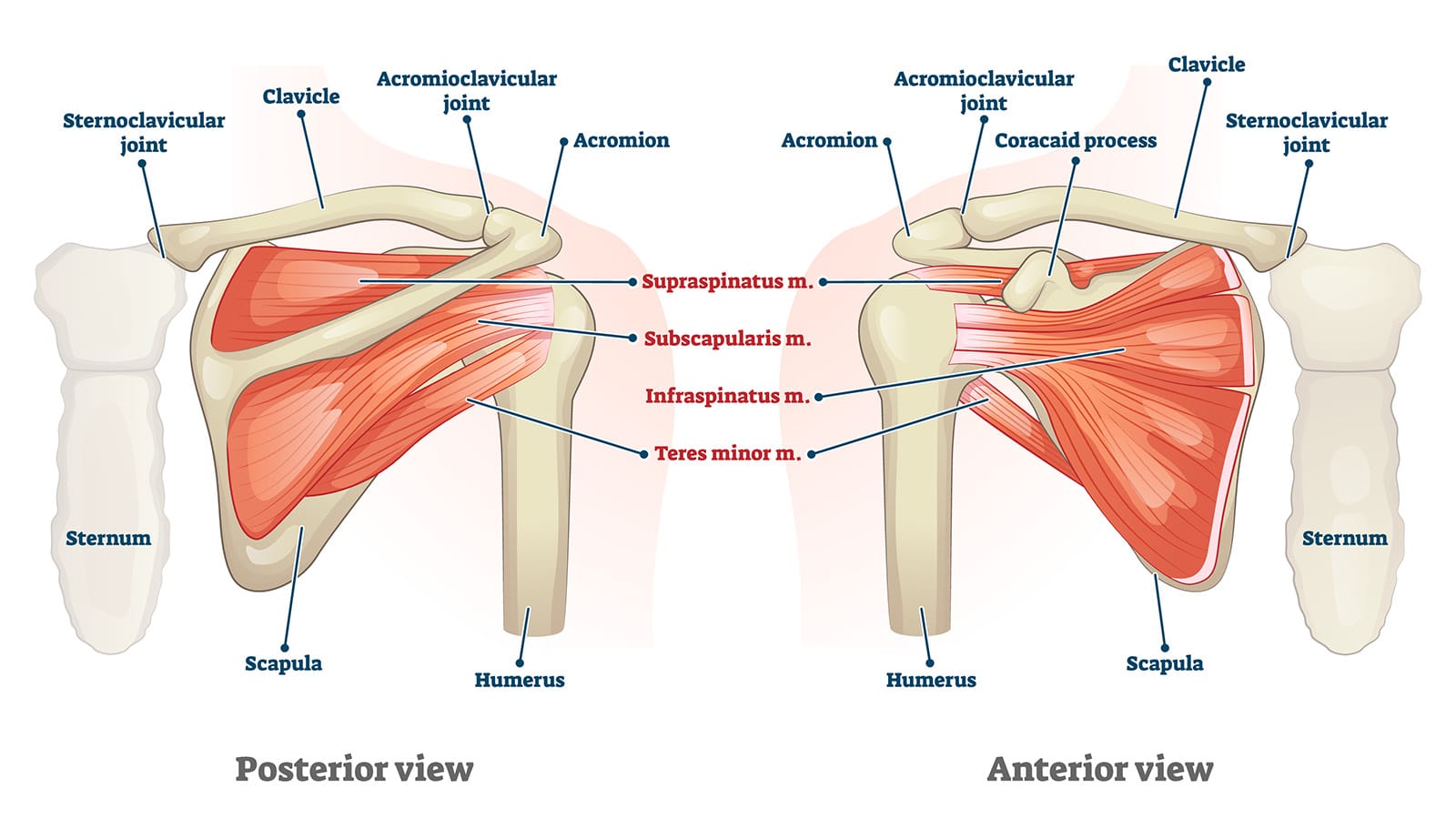
The rotator cuff acts like a team of finely coordinated stabilisers, keeping the ball of the shoulder centred throughout the movement.
The labrum, a ring of cartilage around the socket, deepens the joint and provides stability during the extreme positions required for serving.
The scapula (shoulder blade) acts as the foundation. If it doesn’t move well, the shoulder above it struggles.
Then there are the larger power muscles – the deltoid, pectorals, latissimus dorsi and core – which generate the explosive force that eventually reaches the racket.
When they all work together, serving feels effortless.
When they don’t, the shoulder usually lets you know.
It’s not always the shoulder’s fault
One of the biggest misconceptions I see is that shoulder pain automatically means something is torn.
Fortunately, that’s rarely the case.
Many players arrive convinced they have “done their rotator cuff” after reading online forums or receiving an MRI report full of alarming terminology.
In reality, the shoulder is often the innocent bystander.
Perhaps the thoracic spine has become stiff after long hours at a desk.
Perhaps the hips aren’t generating enough rotation.
Perhaps fatigue has altered serving mechanics after playing three matches in a weekend.
The shoulder simply ends up absorbing loads it was never designed to take.
This is why a proper assessment matters so much.
Rather than focusing solely on the painful shoulder, we look at how the entire body is moving – from the feet all the way to the racket.
Very often, the solution to the problem lies somewhere else.
The patient who couldn’t finish a match
One presentation I see surprisingly often goes something like this.
“I can play for about half an hour…”
“The forehand is fine.”
“The backhand is fine.”
“But once I start serving repeatedly, the pain gradually builds.”
By the third set, serving becomes almost impossible.
Interestingly, everyday activities are often completely normal. Sleeping isn’t a problem. Lifting shopping isn’t a problem.
It’s only the serve.
Why?
Because the serve places the shoulder into its most vulnerable position – maximum external rotation followed by explosive acceleration.
Small weaknesses that go unnoticed during everyday life suddenly become very obvious.
Often this isn’t a major structural injury at all.
It may simply reflect fatigue of the rotator cuff, reduced shoulder blade control, stiffness elsewhere in the kinetic chain or an overload issue after increasing playing time too quickly.
The encouraging news is that these problems frequently respond extremely well to carefully targeted rehabilitation.
More isn’t always better
There’s a saying in sports rehab:
“You don’t get stronger during training – you get stronger while recovering from it.”
Our enthusiasm for tennis can sometimes work against us.
A new racket.
A new coach.
Two tournaments.
Three cardio sessions.
Gym twice a week.
Padel with friends on Sunday.
The shoulder never really gets a day off.
Unlike muscles, tendons adapt relatively slowly. They need gradual increases in loading.
If workload increases faster than tissue capacity, discomfort often follows.
One of the most valuable conversations I have with patients isn’t about surgery.
It’s about training smarter, and rehabilitating fully.
The shoulder is part of a chain
One of the reasons tennis is such a fascinating sport is that the serve isn’t just an arm movement.
In fact, the arm contributes surprisingly little on its own.
Power starts from the ground.
The legs generate force.
The hips rotate.
The trunk transfers energy.
The shoulder accelerates.
The elbow, wrist and racket simply deliver it.
We call this the kinetic chain, and if one link isn’t functioning efficiently, another has to compensate.
A stiff ankle.
Weak gluteal muscles.
Poor core control.
Limited thoracic rotation.
All of these can increase the demands placed on the shoulder.
It’s another reason why successful treatment often involves much more than treating the shoulder itself.
Does shoulder pain always mean surgery?
Thankfully, no.
In fact, most tennis-related shoulder conditions improve without an operation.
A careful diagnosis is essential because not all shoulder pain is the same.
Some people have inflammation of the rotator cuff tendons.
Others develop instability.
Some have irritation of the labrum.
Occasionally, arthritis or larger tendon tears are responsible.
Each requires a slightly different approach.
That’s why imaging is only one piece of the puzzle.
An MRI can reveal age-related changes that may have little or nothing to do with your symptoms.
The scan needs to be interpreted alongside your history, examination and goals.
For many patients, a combination of physiotherapy, activity modification, strength work and occasionally image-guided injections provides excellent results.
Surgery is reserved for situations where conservative treatment hasn’t achieved the desired outcome or where there is a significant structural injury that is unlikely to recover without repair.
A team sport off the court
One aspect of shoulder care that has changed enormously over recent years is how collaborative it has become.
The best outcomes rarely come from one clinician working in isolation.
Sports physicians, physiotherapists, strength and conditioning coaches, radiologists and surgeons all bring different expertise.
As shoulder specialists, our role isn’t simply deciding whether someone needs an operation.
It’s helping each individual find the right pathway to get back to doing what they love—whether that’s competing at Wimbledon, playing in the local club doubles league or simply enjoying a weekly hit with friends.
Sometimes that involves surgery.
Often it doesn’t.
Looking after your most valuable tennis partner
Most players spend hours choosing the perfect racket, restringing their equipment or refining their serve.
Far fewer spend the same amount of time looking after the one piece of equipment they can never replace – their shoulder.
The good news is that the shoulder is remarkably adaptable.
With the right diagnosis, progressive strengthening, sensible workload management and good movement patterns, it can often recover extremely well.
So, the next time you step onto court and fire down an ace, spare a thought for the extraordinary joint that made it possible.
Join 4 members of the London Bridge Orthopaedics team for a CPD accredited talk on their specialist areas. The talk is open to NHS and Private GPs and takes place tomorrow, September 9th from 6 pm. Book your place online. ... Read more